NASA Just Showed Us All How High-Performing Teams Debrief
- Apr 13
- 15 min read
Updated: Jun 7
Author: Paul C. Mullan, MD, MPH, Emergency Medicine Physician
Quality and Patient Safety Leader Affiliation: Advancing Healthcare Debriefing Quality Patient Safety Organization
Published: April 13, 2026 Last Updated: April 17, 2026
A real-time science debrief from orbit shows what frontline learning looks like when it is done well. The Artemis II science debrief had not formally begun when Mission Specialist Jeremy Hansen flagged a gap in his own record-keeping. He had not documented where the crew saw the impact flashes during the lunar flyby. He offered to reconstruct a rough annotation from memory and asked whether it would still be worth anything. Dr. Kelsey Young's response from the ground: "Can you read my mind? This is exactly the first question on our list."
On April 6, 2026, the Artemis II crew completed a seven-hour lunar observation session. Their spacecraft passed within 4,067 miles of the surface, making it the first time humans had traveled to the Moon's vicinity in more than 50 years. The crew included Commander Reid Wiseman, Pilot Victor Glover, and Mission Specialists Christina Koch and Jeremy Hansen. They recorded observations, audio notes, and visual impressions throughout the flyby. Approximately 18 hours later, while still in transit back to Earth, they debriefed with Dr. Kelsey Young and the science team on the ground. The conversation covered impact flashes observed on the lunar surface, possible lofted dust near the horizon, crater features, the Moon's changing appearance as Earth came into view, and the unexpected ways cabin lighting and visual adaptation affected what the crew could actually see. In debriefing practice, this is called a hot debrief: a structured conversation that happens shortly after an event, while the team is still together and the details are still fresh.
Why Timing Is the First Principle of Clinical Debriefing
The first thing to name is timing. It happened approximately 18 hours after the flyby concluded, while the crew was still in space, still close to the sensory experience, before memory had been smoothed by sleep, conversation, or the natural human tendency to tidy up a story.
In debriefing practice, the value of a close-in conversation is that perceptions degrade quickly. Details for the NASA team, such as color, sequence, duration, and spatial location are retrievable within hours of an event. They are not reliably retrievable from a committee room a week later. The Artemis science team understood this limitation. You can hear it in the requests for timing granularity, color descriptions, rough spatial annotations, and duration estimates around the impact flashes. They were not asking out of curiosity. They were trying to preserve the signal before it faded. You can almost hear in their thinking-out-loud voices that they wish they had debriefed even closer to the lunar flyby, not 18 hours later.

Healthcare teams face the same window, and most of the time, they let that critical window of reflection close as well. After a resuscitation, a difficult intubation, or a near miss, the people present hold the most operationally useful information the system is likely to obtain. Their perception of sequence, their sense of what was unclear, their awareness of what nearly went differently: that knowledge is available in the first minutes to hours. It is rarely captured then.
What the Artemis debrief also showed is that asking is not enough on its own. Dr. Kelsey Young and the science team were not simply collecting testimony. They were actively guiding the crew to move from raw observation toward shared interpretation and, eventually, toward a hypothesis. Kelsey named this explicitly, inviting the crew to treat the exchange as a discussion and to move from observation to inference to hypotheses. That is the structural core of a strong clinical debrief as well. It does not stop at what happened. It moves toward what the team thinks it means, and what that creates for the next event.

Eight Debriefing Behaviors the Artemis II Crew Modeled Well
This was, in clinical terms, a hot debrief: a structured conversation that takes place shortly after an event, while sensory detail is still retrievable. In clinical medicine, that usually means within the same shift, before the team disperses and the signal fades. The transcript reveals several specific behaviors that made this NASA debrief aligned well with debriefing best practices.
1. Self-Initiated Delta Questions
"I did not record at all where we saw the impact flashes yesterday... I don't know if that's of any value or not, but if Reid and I can record a rough position in OneNote..."
— Jeremy Hansen, Artemis II Astronaut, before the first formal question
Before any formal question, Jeremy Hansen named what he had failed to capture and immediately proposed a corrective step, known as a delta comment (i.e., what could be changed) in the debriefing nomenclature. He did not wait to be audited. In strong clinical debriefs, one of the highest-yield moments is when someone says unprompted: "I should have called for help sooner" or "we did not order the diagnostic test as early as we could have." That is what ownership of learning looks like from the inside.
2. Structured Sensemaking
"...taking things from observation to inference to hypotheses really added scientific value... please treat it like a discussion."
— Dr. Kelsey Young, NASA Lead Science Officer, Debriefing Facilitator as she opened the debrief
Kelsey Young framed the exchange explicitly as a discussion and invited the crew to move from "observation to inference to hypotheses." Stopping at "the airway was difficult" is an observation. In my experience, debriefing events like intubations in the emergency department, it is when we note the position of team members, the accessibility of the Yankauer suction device, and the lack of a shoulder roll that we reach the details that speak to what should change before the next similar event. That is where the learning lives to improve performance next time.
3. Work-as-Done vs Work-As-Imagined (Concept of Erik Hollnagel)
"I know myself in particular, but probably we all underestimated the amount of impact of sunlight and earth glow on cabin windows, on glare on the window structure... I ended up asking Reid to give me some black T-shirts and we covered all of that stuff so that the reflection was just less in the glass and it worked so well. It basically made observing for impact flashes possible whereas it wouldn't have been otherwise."
— Christina Koch, Artemis II Astronaut,
The science team expected a clean observation task. The crew revealed the operational reality: glare from Earth was more disruptive than anticipated, interior cabin objects shifted color perception, eye adaptation required deliberate time, and a set of black T-shirts became an improvised fix effective enough to recommend for future missions. Clinical debriefs regularly surface the same gaps that require workarounds to keep the patient safe and the team on task. The preparation imagines one method, but the team experiences the sharp end of providing care.
4. Truth Preservation
"My crewmates... they didn't see it the same as I did."
— Christina Koch, Artemis II Astronaut, on possible lofted dust
"Negative. Just really wanted to see some and I saw none."
— Reid Wiseman, Artemis II Astronaut, on suspended dust
Christina Koch described possible lofted dust that her crewmates did not see the same way. Reid Wiseman looked deliberately for suspended dust and found none. Neither observation was erased to produce a tidy account. Good clinical debriefs work the same way: one nurse noticed confusion in medication preparation, a physician did not, and a pharmacist interpreted it differently. The goal is disciplined comparison of what each person actually experienced, not instant agreement.
5. Real-Time Leadership
"We definitely want that annotation. Please let us know when you have that, and we'll try to downlink it in flight."
— Dr. Kelsey Young, NASA Lead Science Officer, Debriefing Facilitator
When crew members described how glare and cabin reflections disrupted observation, the science team did not log it for a future committee review. They probed further, requested in-flight annotations, and treated the feedback as design input for future missions. In many healthcare organizations, the gap between frontline experience and institutional response is measured in weeks. By then, the details have blurred, and the people closest to the event have moved on to other concerns. When leaders later provide a closed-loop communication back to the team on the actions taken from their insights, it reinforces the value of the debriefing.
6. Bias Without Paralysis
"And maybe it was a priming bias, but to me there was no doubt we were seeing it. And we were all seeing it."
— Reid Wiseman, Artemis II Astronaut, on the impact flashes
This is a high-level debriefing move, and it is rarely modeled this cleanly. Reid names a potential cognitive distortion, the possibility that expectation shaped perception, then offers his judgment anyway, grounded in shared crew corroboration. Good clinical debriefs are not about pretending bias does not exist. They are about surfacing it while still preserving the observation. A clinician who says "I know I was anchoring on sepsis early, but I still think the blood pressure trend was concerning" is doing exactly the same thing.
7. Memory and Dialogue
"The picture I'm building in my mind, I just want to make sure I'm not, like, creating false memories."
— Christina Koch, Artemis II Astronaut,
This may be the most clinically sophisticated line in the transcript. It shows an understanding that memory is reconstructive, that post-event discussion can distort recall as easily as it can clarify it, and that people can inadvertently overfit a narrative to what they expect to have happened. The answer the crew modeled was not silence. It was careful dialogue: compare perspectives, preserve uncertainty, and refine the account without inventing one. Debriefing is not valuable because memory is perfect. It is valuable because teams can compare imperfect memories quickly enough to recover something more useful than any one person's reconstruction alone. In our research, we found that teams had a median accuracy of 90% during hot debriefings of resuscitations and that their accuracy improved over time as they conducted debriefings.
8. Psychological Safety
"Kelsey, love all those words."
— Jeremy Hansen, Artemis II Astronaut, responding to the facilitator's framing
"Oh, we're not on video. This whole time I've been sitting on the show. I was nodding..."
— Christina Koch, Artemis II Astronaut,
The humor in this debrief was not incidental. When Christina joked about nodding vigorously on audio-only, the conversation opened rather than contracted. When Jeremy responded to Kelsey's framing with warmth, it set the tone for what followed. These moments signal that the debrief was rigorous without being rigid. The best clinical debriefs have the same quality. People speak more freely, admit more honestly, and contribute more usefully when the tone makes them feel safe. Humor is often injected into many debriefs I have led or participated in, and it brings the team closer together. Psychological safety does not always look solemn.

Three Practice Implications for Clinical Debriefing Teams
1) Data-Dialogue Gap
The Artemis debrief is a useful reminder that data and dialogue do different things. The crew already had audio notes, photographs, and recordings from the flyby. The live conversation still added what those inputs could not: the chance to probe for perception, sequence, disagreement, and the improvised workarounds that never appear in a formal record. In healthcare, incident reports and chart reviews remain worthwhile when required. They are not sufficient on their own. They rarely capture what team members perceived, what they adapted to in real time, or what they knew but did not document. A structured debriefing program can help to close that gap.
2) Debriefing Facilitation
The facilitator's role matters more than most debrief training suggests. Kelsey Young's repeated use of phrases like "that's great feedback" was not filler. It kept the crew elaborating. It rewarded useful observations in real time and directed the conversation toward actionable detail. A clinical debrief facilitator is not a neutral recorder. Oftentimes, when documenting on paper or electronic debriefing tools, they are the ones recording the team's input. Most times, they were also participants on the clinical team for the event as well. They actively shape what gets surfaced and what stays hidden.
3) Debrief Timing
Timing is a leadership decision, not a circumstance. Hot debriefs do not happen by accident. Someone has to protect the time for a few minutes, keep the team together before they disperse, and signal that the conversation is worth having. The Artemis science team built this into the mission schedule. Clinical teams that debrief consistently do the same: they make it structural, not optional, and treat it as a standard part of how complex work gets done.
Five Questions to Ask Your Team In the Debrief Before They Leave the Room
These questions are designed for use immediately after a critical clinical event, while the team is still together and the detail is still fresh. In my experience, they take five to ten minutes, or can be done in two to three minutes if covering only the first two questions.
1. What did we do well as a team? (Plus-question)
2. What do we wish we had done differently? (Delta-question)
3. Did anyone see anything differently, or notice something the rest of the team may have missed?
4. Were there any workarounds we used to accomplish any tasks?
5. What things should we address before the next similar event?
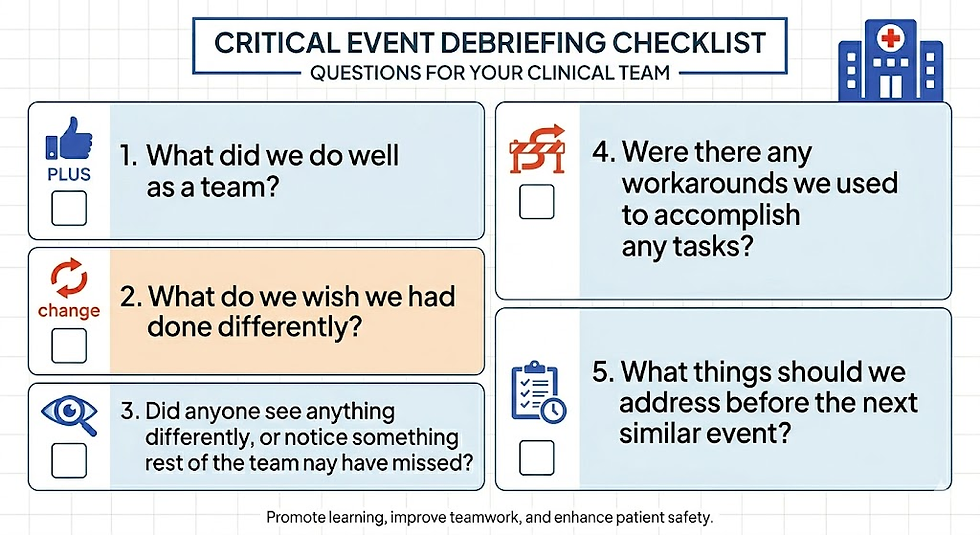
The first question establishes a constructive tone and reminds the team that learning includes what worked, not only what did not. The second creates space for voluntary delta sharing, the most high-yield moment in any debrief. The third protects against false consensus by inviting perspectives the group may not have heard. The fourth captures improvised adaptations before they disappear from memory. The fifth closes with a forward-facing commitment, anchoring the conversation in what the team will actually do before the next similar event. Determining the right questions to ask in a debriefing tool requires leaders to design clinical debriefing programs with a global blueprint in mind.

Closing Thoughts
Near the end of the debrief, one line stood out: "This was too short." It was not a complaint. It was an acknowledgment that even a focused, well-run conversation cannot exhaust all the discoverable lessons a complex event has to teach. That is almost always the case. Notice what they did not say: "The debrief is too long." What I keep returning to is not whether clinical debriefs are too short, but why they so rarely happen at all before the team disperses, the shift changes, and the learning that was available at the bedside an hour ago is no longer recoverable.
There is a small but growing community of us who work in post-event debriefing to improve the quality and safety of healthcare delivery. We are studying how debriefs are implemented, collaborating across disciplines, advocating for increased adoption with World Debriefing Day and other initiatives, innovating the structures that make them reliable, and building evidence that connects structured reflection to outcomes that matter to patients, teams, and the organizations that care for them. The goal is related to the same one that sent four people around the moon on the Artemis II mission. If we are willing to explore this frontier of debriefing science in healthcare, we can go farther in team performance than we have ever gone before.
FAQ Section: Clinical Debriefing After Critical Events
Q: What is a hot debrief in healthcare?
A hot debrief in healthcare is a brief, structured conversation that happens soon after a clinical event, while the team is still together and the details are still fresh. It is designed to capture what went well, what could be improved, what different team members noticed, and what should change before the next similar event.
Q: When should a clinical team debrief after a critical event?
A clinical team should debrief as soon as practical after the event, ideally within the same shift and before the team disperses. The closer the conversation is to the event, the more likely the team is to recall important details such as sequence, communication challenges, workarounds, and near misses.
Q: How long should a clinical debrief take?
Most clinical hot debriefs can be completed in about 5 to 10 minutes. In busy environments, a shorter 2- to 3-minute version can still be valuable if the team focuses on the highest-yield questions and captures one or two actionable takeaways.
Q: What is the difference between a clinical debrief and an incident report?
A clinical debrief is a live team conversation that captures frontline perspectives shortly after an event. An incident report is usually an individual, documented report submitted later through a formal system. Incident reports are useful, but they often miss real-time observations, team dynamics, workarounds, and differences in perception that can emerge in a debrief.
Q: What questions should I ask in a post-event clinical debrief?
A simple post-event debrief can include questions like: What went well? What do we wish we had done differently? Did anyone notice something others may have missed? Were there any workarounds? What should we change before the next similar event? These questions help teams move from observation to action.
Q: Who should participate in a healthcare debrief after an event?
The best participants are the people directly involved in the event or closely observing it, as long as they are available. This often includes physicians, nurses, respiratory therapists, pharmacists, technicians, and others who contributed to the care. The goal is to hear the voices closest to the work as it was actually done.
Q: What is the goal of a clinical debrief?
The goal of a clinical debrief is not to assign blame. It is to help the team learn quickly from real clinical work, improve future performance, identify system issues, reinforce effective behaviors, and strengthen patient safety, teamwork, and operational reliability.
How this article was created
This article is based on direct analysis of the NASA Artemis II Day 7 science debrief transcript (April 7, 2026), peer-reviewed research in clinical debriefing, and more than a decade of real-world implementation experience across healthcare systems across the globe. The clinical parallels and practice observations reflect the author's own research and frontline debriefing work.
Additional Resources
If you want to dive deeper into debriefing and understand the evidence, theoretical frameworks, and step-by-step implementation pathway, then The Clinical Debriefing Guide is your comprehensive resource. If you are building the case for a structured debriefing program at your healthcare organization, a debriefing ROI Calculator can help you quantify the business case. If you want to score the current state of whether your healthcare organization has a high-reliability organization system in place for debriefing, take this 2-minute SAFER Framework assessment. If you are starting or strengthening a clinical debriefing program, have your team answer these 50 critical questions to establish a strong program blueprint. If your healthcare organization is looking to join a Patient Safety Organization to ensure that debriefing data is both protected and to learn from other like-minded professionals how to debrief smarter to improve faster, learn about the AHDQ PSO, the only PSO solely focused on debriefing.
References
National Aeronautics and Space Administration. (2026, April 1). Artemis II press kit. NASA. https://www.nasa.gov/artemis-ii-press-kit/
Barry, R. (2026, April 3). Meet NASA’s new Artemis II science officers. NASA Science. https://science.nasa.gov/missions/artemis/meet-nasas-new-artemis-ii-science-officers/
Agency for Healthcare Research and Quality. (2023, December). Reviewing the team’s performance: Debrief. U.S. Department of Health and Human Services. https://www.ahrq.gov/teamstepps-program/curriculum/team/tools/debrief.html
Agency for Healthcare Research and Quality. (2023, August). TeamSTEPPS video: Debrief in emergency department. U.S. Department of Health and Human Services. https://www.ahrq.gov/teamstepps-program/resources/additional/debrief-ed.html
American Heart Association. (2023, March 2). Get With The Guidelines®–Resuscitation clinical tools: Hot debriefing form examples. https://www.heart.org/en/professional/quality-improvement/get-with-the-guidelines/get-with-the-guidelines-resuscitation/get-with-the-guidelines-resuscitation-clinical-tools
Baker, A. C. L., Monuteaux, M. C., Mullan, P. C., Nagler, J., & Dorney, K. (2025). Simulation-based training in clinical event debriefing improves leadership performance. Pediatric Emergency Care, 41(2), 86–93. https://pubmed.ncbi.nlm.nih.gov/39509323/
Coggins, A., De Los Santos, A., Zaklama, R., & Murphy, M. (2020). Interdisciplinary clinical debriefing in the emergency department: An observational study of learning topics and outcomes. BMC Emergency Medicine, 20, 79. https://pmc.ncbi.nlm.nih.gov/articles/PMC7542715/ Edmondson, A. (1999). Psychological safety and learning behavior in work teams. Administrative Science Quarterly, 44(2), 350–383. https://doi.org/10.2307/2666999
Hollnagel, E. (2014). Safety-I and Safety-II: The past and future of safety management. Ashgate. https://erikhollnagel.com/books/safety-i-and-safety-ii.html Kessler, D. O., Cheng, A., & Mullan, P. C. (2015). Debriefing in the emergency department after clinical events: A practical guide. Annals of Emergency Medicine, 65(6), 690–698. https://pubmed.ncbi.nlm.nih.gov/25455910/ Light, T., Hamilton, T., & Pfeifer, S. (2020). Trends in U.S. Air Force aircraft mishap rates (1950–2018) (RR-A257-1). RAND Corporation. https://www.rand.org/pubs/research_reports/RRA257-1.html
Mullan, P. C., Wuestner, E., Kerr, T. D., Christopher, D. P., & Patel, B. (2013). Implementation of an in situ qualitative debriefing tool for resuscitation. Resuscitation, 84(7), 946–951. https://pubmed.ncbi.nlm.nih.gov/23266394/ Mullan, P. C., Kessler, D. O., & Cheng, A. (2014). Educational opportunities with postevent debriefing. JAMA, 312(22), 2333–2334. https://pubmed.ncbi.nlm.nih.gov/25490319/ Mullan, P. C., Cochrane, N. H., Chamberlain, J. M., Burd, R. S., Jacobs, B. R., Noviski, N., & Cheng, A. (2017). Accuracy of postresuscitation team debriefings in a pediatric emergency department. Annals of Emergency Medicine, 70(3), 311–319. https://pubmed.ncbi.nlm.nih.gov/28259482/ Mullan, P. C., Zinns, L. E., & Cheng, A. (2021). Debriefing the debriefings: Caring for our patients and caring for ourselves. Hospital Pediatrics, 11(12), e412–e414. https://pubmed.ncbi.nlm.nih.gov/34807984/
Mullan, P. C., Zinns, L. E., & Cheng, A. (2021). Debriefing the debriefings: Caring for our patients and caring for ourselves. Hospital Pediatrics, 11(12), e412–e414. https://publications.aap.org/hospitalpediatrics/article/11/12/e412/183404/Debriefing-the-Debriefings-Caring-for-Our-Patients Mullan, P. C., Jennings, A. D., Stricklan, E., Greenberg, R. A., Eagle, C. A., Channing, J., Hines, L. P., Horowitz, D., & Mullan, M. (2023). Reducing physical restraints in pediatrics: A quality improvement mixed-methods analysis of implementing clinical debriefing process after behavioural health emergencies in a Children’s Hospital. Current Problems in Pediatric and Adolescent Health Care, 53(10), 101463. https://pubmed.ncbi.nlm.nih.gov/38000959/
Sawyer, T., Loren, D., & Halamek, L. P. (2016). Post-event debriefings during neonatal care: Why are we not doing them, and how can we start? Journal of Perinatology, 36(6), 415–419. https://pubmed.ncbi.nlm.nih.gov/27028072/
Sweberg, T., Sen, A. I., Mullan, P. C., Cheng, A., Knight, L., Leary, M., Abella, B. S., & Nadkarni, V. M. (2018). Description of hot debriefings after in-hospital cardiac arrest in an international pediatric quality improvement collaborative. Resuscitation, 128, 181–187. https://pubmed.ncbi.nlm.nih.gov/29768181/
Tannenbaum, S. I., & Cerasoli, C. P. (2013). Do team and individual debriefs enhance performance? A meta-analysis. Human Factors, 55(1), 231–245. https://pubmed.ncbi.nlm.nih.gov/23516804/
HOW TO CITE THIS ARTICLE
Mullan PC. NASA Just Showed Us All How High-Performing Teams Debrief. StatDebrief. Published April 13, 2026. Accessed [insert date]. https://www.statdebrief.com/post/how-high-performing-teams-debrief
About the Author
Dr. Paul Mullan, MD, MPH is an emergency medicine physician and patient safety leader with over 15 years of experience implementing clinical event debriefing programs in hospitals worldwide. He is the founder of StatDebrief and leads the AHDQ Patient Safety Organization (www.ahdq.org), an AHRQ-listed PSO focused on improving learning after clinical events. https://www.linkedin.com/in/drpaulmullan/


Comments