The Clinical Debriefing Guide: What Every Patient Safety Leader Should Know (2026)
- May 11
- 44 min read
Updated: Jun 10
Author: Paul C. Mullan, MD, MPH, Emergency Medicine Physician
Quality and Patient Safety Leader | AHDQ Patient Safety Organization Leader
Published: May 5, 2026
Last updated: May 5, 2026
Organization: AHDQ Patient Safety Organization — AHRQ-listed PSO
What Is Clinical Debriefing?
Clinical debriefing is a structured, reflective conversation held after a real patient care event to help healthcare teams identify opportunities for improvement and improve future outcomes. It serves as a universal safety mechanism, adaptable to any clinical environment to foster a culture of continuous, real-time learning. Unlike simulation debriefing, which uses a controlled environment to build individual or team competency, clinical debriefing engages directly with the complexity of actual events to surface systemic gaps, reinforce high-performance teamwork, and drive measurable improvements in care delivery. It is not a psychological intervention, a performance review, or a replacement for formal incident reporting.
Why this matters:
• Debriefings evaluate team collaboration and systems thinking, not just individual performance
• Debriefings are a core practice of high-reliability organizations that maintain sensitivity to operations and uphold a commitment to resilience
• Hospitals and clinics without structured programs miss opportunities to reduce preventable harm
• Structured debriefing programs reduce workforce burnout and support staff after difficult events
Quick Summary
What is clinical debriefing in practice? It is a structured team conversation held after a clinical event to identify what went well, what broke down, and what needs to change.
Does it actually improve patient safety? Evidence from emergency medicine, critical care, and pediatric settings shows that consistent debriefing programs reduce the recurrence of adverse events, improve team communication, and support a strong safety culture.
Is it sustainable for busy clinical teams? Yes, when built on a tiered model that aligns debrief depth and format with event type and severity.
Is your debriefing program built to last? Most hospitals have some form of event review, but few have a structured, consistent debriefing program that produces learning at the unit level. AHDQ PSO offers a free Debriefing Program Readiness Assessment to help you identify gaps before they become system failures. Take the Free SAFER Debriefing Readiness Assessment |
WHAT THIS ARTICLE COVERS
INTRODUCTION
Patient harm still occurs in well-staffed, well-resourced hospitals. It happens not because clinicians lack skill or commitment, but because teams rarely have a structured way to learn from what just occurred during their shift. An event ends, the team disperses, and the conditions that shaped it remain unchanged. The next shift begins with the same latent risks in place.
Clinical debriefing exists to close that gap. It is the practice of pausing after a patient care event to ask three questions as a team: what happened, why it happened, and what we will do differently. When done consistently and with structure, it is one of the most practical tools available to hospital quality and safety leaders for effective healthcare debriefing at the unit level and organizational levels.
Debriefing is now recommended by AHRQ, The Joint Commission, American Heart Association, and many others. The evidence for clinical debriefing spans from early resuscitation research to large-scale analyses of team performance across various clinical care settings. Over 15 years of work implementing and studying debriefing programs across emergency departments, ICUs, and other hospital areas show that the gap between knowing debriefing works and actually sustaining a program is where most organizations struggle. This article addresses both sides of that equation.
What follows is a practical, evidence-based guide for hospital quality directors, patient safety officers, risk managers, and clinical leaders who want to build or strengthen a clinical debriefing program. It covers the evidence base, operational mechanics, theoretical frameworks, common failure points, and a step-by-step implementation path. It is written for leaders who need to act, not just understand, to optimize the effectiveness of their debriefing program.
What Is the Current State of Clinical Debriefing in Hospitals?
The current state of clinical debriefing in hospitals is inconsistent and largely champion-dependent: most institutions have some form of event review, but fewer than half have a structured debriefing program, and among those that do, debriefing occurs after only a minority of qualifying events. The Institute of Medicine's landmark 1999 To Err is Human report estimated that up to 98,000 Americans die annually from preventable medical errors, and progress toward eliminating that harm has been slower than the patient safety field hoped. A 2019 assessment found that while effective interventions exist, successful implementation remains inconsistent across hospital settings. Clinical debriefing is one of the most practical yet underused of the many innovative approaches to enhancing patient safety.
Why Most Hospitals Debrief Inconsistently or Not at All
Why do so few hospitals consistently debrief after clinical events? The fundamental reason is that debriefing was never formally integrated into the clinical workflow. It was introduced as a good idea, modeled occasionally by enthusiastic champions, and then gradually abandoned as competing priorities filled the space it had occupied. In high-reliability organizations such as aviation or nuclear power, teams routinely debrief after events as part of their workflow.
A national survey of pediatric emergency departments found that fewer than half of respondents reported having a formal debriefing program, and among those that did, debriefing occurred after only a minority of qualifying events. A 2024 systematic review confirmed that implementation has remained highly variable across acute care settings, with most programs dependent on individual champions rather than a codified structure. Debriefing happens when someone remembers to do it, not because a system has a reliable method that ensures it will be done.
The result is a learning gap that compounds over time. Teams that do not debrief consistently fail to build the shared mental models and psychological safety that make future debriefs even more productive. Programs that start informally tend to drift toward less activity over time.
What Clinical Debriefing Is Not
Clinical debriefing is not a psychological intervention, a performance review, an incident report, or a replacement for formal disciplinary processes, but conflating it with any of these things is one of the most common barriers to successful program adoption. Clinical debriefing is often confused with other clinical review, support, and accountability processes; the distinctions below clarify its unique purpose in patient safety and team learning. Table 1. Clinical Debriefing Compared With Other Healthcare Quality Activities
Process | Primary Purpose | Typical Facilitator | Typical Timing | Primary Output |
Clinical Debriefing | Team learning and systems improvement after a real patient care event | Attending, charge nurse, or trained team lead | Immediately within minutes to hours after an event | Actionable learning, shared mental model, referral if needed |
Simulation Debriefing | Skill and competency development after a scripted training exercise | Simulation educator or trained facilitator | Immediately after the simulation scenario | Individual and team competency improvement |
Critical Incident Stress Debriefing (CISD) | Psychological intervention to reduce post-traumatic stress after traumatic exposure | Mental health professional or trained CISD facilitator | 24-72 hours after a critical incident | Emotional processing, trauma mitigation, referral to care |
Psychological First Aid | Immediate emotional stabilization after acute distress | Any trained responder, peer supporter, or leader | Immediately after the event | Stabilization, connection to resources |
Incident Reporting | Formal documentation of a safety event for tracking and analysis | Individual reporter (any staff member) | Within hours to days of the event | Event record, trend data, regulatory compliance |
M&M Conference | Retrospective case review for educational and quality purposes | Department chief or quality leader | Days to weeks after the event | Educational learning, quality improvement recommendations |
Root Cause Analysis (RCA) | Deep systems analysis of a sentinel event | Quality or patient safety team | Days to weeks after the event | Systems-level findings, corrective action plan |
Just Culture Review | Evaluation of individual behavior in context of system factors | Risk management, HR, quality leadership | Following RCA or serious event review | Behavioral accountability decision, system improvement action |
Three distinctions deserve particular emphasis. Clinical debriefing and CISD serve fundamentally different purposes. CISD is a structured psychological intervention for trauma mitigation facilitated by mental health professionals. A Cochrane review found no evidence that single-session CISD prevents PTSD after trauma, with some evidence of possible harm. Clinical debriefing is also not a substitute for formal incident reporting. The two processes are complementary, and high-functioning safety programs deliberately integrate them.
The Gap Between Events and Learning
Healthcare settings generate a large volume of safety-relevant events every day. Most of them are never reported and do not yield learning at the unit level. Incident reporting systems capture only a fraction of events, and even reported events often move through review processes that take days to weeks to produce feedback that reaches the frontline team.
Clinical debriefing addresses a specific and underserved part of the learning cycle: the immediate window after an event, when team members' observations are fresh, emotions are present, and the conditions that shaped the event are still visible. Work as done, rather than work as imagined, is the data source that clinical debriefing captures best. Debriefing surfaces that gap in real time, before the opportunity for learning disappears.
Cultural and Structural Barriers That Stall Programs
The most common structural barrier cited in clinician surveys is limited time. Clinicians working at capacity in high-acuity environments lack a built-in pause in their workflow for reflection. Without a designated trigger, a defined format, and explicit leadership support, debriefing competes with every other demand on clinical time.
The most common cultural barrier is psychological safety in healthcare teams. Team members will not speak candidly in a debrief if they fear that what they say will be used against them. Psychological safety is not a fixed team characteristic. It is a condition that leaders create or fail to create through their behavior before, during, and after every debrief. Organizations that have tried and abandoned debriefing programs most often cite three failure modes that contributed to the failure: lack of institutional support, lack of documentation, and a weak or nonexistent feedback loop.
Assess your debriefing readiness in 2 minutes — get your baseline score |
What Does the Evidence Show About Clinical Debriefing?
The evidence shows that structured clinical debriefing consistently improves team performance, supports safety culture, and reduces preventable events. The strongest data links debriefing programs to improvements in processes, changes in team behavior, and measurable patient outcomes across emergency medicine, critical care, and pediatric settings.
Landmark Studies and What They Demonstrate
What does the research show about debriefing effectiveness? One of the most-cited quantitative studies comes from a 2013 meta-analysis by Tannenbaum and Cerasoli, which analyzed 46 studies across military, aviation, and healthcare settings and found that teams that debrief consistently outperform those that do not by an average of 25 percent. That figure has been widely cited because it quantifies what clinicians intuitively know: structured reflection after performance improves future performance.
A useful framework for organizing the evidence is Donabedian's structure-process-outcome model. Applied to debriefing, a standardized, evidence-based structure increases both the quantity and quality of debriefings. Layering in Michael Porter's value equation, debriefing improves the value of care by simultaneously improving outcomes and reducing costs through less risk and less waste.
The Debriefing Flywheel: How Benefits Compound Across Four Domains
Evidence from peer-reviewed publications demonstrates that healthcare organizations that adopt structured debriefing achieve benefits across all four domains of structure, process, outcomes, and value. Each improvement reinforces the others, creating a flywheel effect that accelerates as program maturity increases.
Figure 1. The Clinical Debriefing Flywheel: How Program Benefits Compound Across Outcomes. Structured clinical debriefing programs can reinforce improvement across five linked domains: process improvement, patient outcomes, teamwork outcomes, team member outcomes, and financial viability.

Teamwork outcomes. In a New York City PICU, a debriefing program resulted in 62 percent of providers reporting improved communication quality during cardiac arrests within twelve months. A survey of emergency nurses found that a higher frequency of clinical event debriefing was associated with increased trust, teamwork, and shared mental modeling. In the surgical setting, a structured debriefing program was associated with the proportion reporting a good safety climate more than doubling, from 42 to 90 percent.
Process improvements. A debriefing program after intubations in a pediatric ED in Melbourne increased first-attempt intubation success from 49 to 78 percent. In an Israeli obstetrics ward, a debriefing program decreased time to emergent cesarean section by 43 percent and improved neonatal outcomes.
Patient outcomes. At McLeod Regional Medical Center in South Carolina, structured debriefing after every OR case was associated with a 33 percent reduction in 30-day surgical mortality. In a pediatric ED in Norfolk, Virginia, debriefing was associated with an 82 percent reduction in physical restraint time for behavioral emergencies. At the Children's Hospital of Philadelphia, an interdisciplinary ICU debriefing program was associated with nearly doubling favorable neurologic outcomes after cardiac arrest, from 29 to 50 percent.
Team member outcomes. A survey of emergency physicians identified institutional debriefing practices as one of five factors that mitigated the impact of burnout on patient outcomes. A large international survey across 24 countries found that teams that debriefed after resuscitations were less likely to report intention to leave their jobs. Clinical debriefing has not been shown to increase PTSD risk, and most participants report feeling generally better after debriefing.
Financial viability. The Rose surgical debriefing program reduced surgical labor hours per case, yielding $4 million in annual savings. Use the debriefing ROI calculator to estimate the financial impact of a debriefing program at your institution. Debriefing has the highest impact when it is integrated with other tools to improve operational efficiency in healthcare.
Use the 10-second debriefing ROI calculator to estimate the financial impact of a debriefing program at your institution. |
History of Debriefing and Its Translation to Medicine
Debriefing as a structured practice did not originate in healthcare. Its roots lie in military after-action reviews and aviation's crew resource management training in the 1970s and 1980s, following catastrophic accidents attributed to communication breakdowns and hierarchy-driven errors in the cockpit. High-reliability organizations such as NASA conduct routine debriefs with their astronaut teams to keep astronauts safe in space.
Healthcare drew on these debriefing traditions, initially through simulation education. Frameworks such as PEARLS and the 3D model were developed for scripted scenarios but do not translate directly to clinical debriefing after real events. Clinical debriefs occur under time pressure, with emotional weight, and with unpredictable team composition.
Recommendations to Debrief by Leading Organizations
Many organizations recommend clinical debriefing, including the American Heart Association, Joint Commission, CMS, ASHRM, American Academy of Pediatrics, and the Institute for Healthcare Improvement. The 2025 American Heart Association Guidelines for CPR and Emergency Cardiovascular Care issued a new treatment recommendation: post-event debriefing is now suggested after adult, pediatric, and neonatal cardiac arrest in all settings.
Table 2. Key 2025 AHA CPR Guideline Updates Relevant to Clinical Debriefing
Debriefing Recommendation | Evidence, Rationale, or Program Implication |
Use both hot and cold debriefs as complementary approaches | Hot debriefs capture fresh team observations immediately after the event; cold debriefs add objective data and allow broader participation and deeper systems analysis |
Use objective data to improve debriefing accuracy, but do not require it | Research shows resuscitation teams achieved 96% recall accuracy on intubation questions and 89% accuracy on CPR epinephrine timing; accuracy improved further as teams debriefed more consistently over time. |
Include nurses, physicians, respiratory therapists, and all available team members in debriefings | Interdisciplinary participation breaks down silos, increases the volume and diversity of input, and produces stronger teamwork in future events |
Use debriefing to support team wellbeing, not just performance improvement | The 2025 guidelines explicitly recognize that debriefings provide a safe space for discussion and allow acknowledgment of the natural stressors associated with caring for cardiac arrest patients |
Beyond cardiac arrest: the Joint Commission recommends debriefing after severe maternal hemorrhage. CMS regulations and ASHRM call for debriefing after inpatient restraint and seclusion events, which have been found to reduce the incidence of restraint events. The American Academy of Pediatrics recommends post-event debriefing to identify opportunities for improvement. The IHI identifies briefings and debriefings as foundational team behaviors in its Framework for Safe, Reliable, and Effective Care.
Why Does Clinical Debriefing Matter in Real Clinical Environments?
Clinical debriefing matters in real clinical environments because it reduces patient harm, decreases workforce burnout, surfaces latent safety threats before they cause injury, and builds the team communication infrastructure that high-reliability organizations depend on. Clinical debriefing occurs within the constraints of real clinical workflow.
Impact on Patient Outcomes and Event Recurrence
Does clinical debriefing actually reduce patient harm? Yes. Structured debriefing programs have been associated with many improved outcomes, including reduced surgical mortality, improved neurologic survival after cardiac arrest, fewer physical restraints, and faster team performance times across multiple care settings. A 33% reduction in 30-day surgical mortality and a near-doubling of favorable neurologic outcomes represent the kind of performance shift that hospital boards and quality committees track as top-tier institutional priorities.
The evidence also shows that outcomes improve most when debriefing is consistent, structured, and integrated into a feedback loop. The distinction between episodic debriefing and programmatic debriefing is the difference between a one-time intervention and a high-performing learning system. Documentation and closed-loop communication in healthcare are the mechanisms through which debriefing converts conversation into measurable harm reduction.
Workforce Burnout, Moral Injury, and the Second Victim Phenomenon
How does clinical debriefing affect the healthcare workforce? Structured debriefing programs are linked to lower burnout, lower intention to leave, reduced moral injury following difficult events, and no increased risk of PTSD among participating clinicians.
Clinicians who participate in difficult clinical events are at risk for what researchers have termed the second victim phenomenon: the psychological distress experienced by healthcare providers after their involvement in an adverse or traumatic patient event. Studies estimate that 10 to 43 percent of healthcare workers experience significant distress after adverse events. Clinical debriefing creates a structured opportunity for teams to process what happened together, normalize the emotional weight of difficult events, and identify colleagues who may need referral to additional support. For hospital executives managing recruitment and retention costs, these findings represent a return on investment that extends well beyond the clinical quality domain. Use the debriefing ROI calculator to model the workforce retention impact at your institution.
Latent Safety Threats and What Debriefing Surfaces
One of the most under-appreciated functions of clinical debriefing is its ability to surface latent safety threats: conditions embedded in the work environment, equipment, workflows, or team culture that become apparent only during a clinical event. Latent safety threats differ from active errors in that they are systemic rather than individual. They do not appear in incident reports until someone connects the dots by recognizing the underlying conditions that degrade safety and quality.
A team debriefing after a difficult intubation may identify that the difficult airway cart is stored in a location that costs two minutes of retrieval time under pressure. A team debriefing after a medication delay may surface a communication gap that repeats itself on every shift. After more than 15 years of clinical debriefing research across multiple clinical settings, the latent safety threats identified in debriefs have consistently outnumbered active errors.
Team Communication, Incident Reporting, and Organizational Culture
How does debriefing affect the broader safety culture of a hospital unit? Regular debriefing strengthens safety culture by building shared mental models, normalizing incident reporting, and creating teams with psychological safety that empower everyone to speak up readily to improve future care.
Teams that debrief regularly develop shared mental models of how their unit operates, the common failure points in patient care, and how to communicate under pressure. Debriefing can also improve incident reporting rates, because staff feel safer identifying problems without fear of blame. That increase in reporting is a sign of a healthier safety culture, not a worsening one.
Case Vignette: An emergency department in a mid-sized community hospital experienced three medication delay events over six months. Each was reported individually. None triggered a formal review. After implementing a structured debriefing program, the team conducted its first debriefing after the fourth event. Minutes into the debrief, a nurse identified a workflow bottleneck: a single medication scanning station was shared between two patient rooms. The fix required an inexpensive additional scanning station. No further medication delay events were reported in the following eight months. The debrief did not discover a new problem. It created the conditions for the team to name a problem they had all noticed but never had a structured opportunity to report. |
How Do You Conduct a Clinical Debrief?
A clinical debrief follows five operational parameters: identify who attends and leads it, define which events trigger a debrief, establish where the debrief occurs, determine the timing of the debrief after the event, and run the conversation using a structured debriefing tool. Knowing that debriefing works is not the same as knowing how to do it. This section answers each question directly and provides the tools to move from intention to execution.
Who Attends and Who Leads a Clinical Debrief?
Who should attend a clinical debrief, and who should lead it? The right participants are those directly involved in the event, and the right facilitator has the interpersonal credibility to foster a psychologically safe conversation on that team.
Attendees should be self-selected from among the event participants who are available and able to share their insights. Participation should be voluntary in most circumstances. The facilitator is usually someone who was a member of the clinical team for the event, but they are not always the most senior person in the room. What matters is not the title but the behavior: opening the conversation, holding the structure, managing the emotional temperature, and ensuring every team member has a chance to contribute. Physicians or unit leaders who lead debriefs should be mindful of hierarchy dynamics, as team members might speak more candidly when leaders explicitly signal that the conversation is not for evaluation but to improve quality and safety.
What Events Should Trigger a Clinical Debrief?
What events should trigger a clinical debrief? Any routine or non-routine event in healthcare could trigger a clinical debrief. By standardizing one or more debriefing triggers within a specific unit, team members can anticipate when to start the debrief, formulate their input more efficiently, and improve their participation rate.
Leaders should determine triggers based on local quality, safety, or risk priorities, in consultation with frontline teams, to ensure relevance and buy-in. Whether to make debriefing mandatory depends on the program's unique design and the clinical environment. New programs should be careful not to aim to debrief 100 percent of their trigger events, as mandating strict compliance with debriefing all trigger events can lead to disengagement.
Table 3. Example Clinical Events That May Trigger a Debriefing by Care Setting
Clinical Setting | Routine Events To Debrief | Non-Routine Events To Debrief |
Ambulatory Surgery Center | Pre-procedure timeout, Patient discharge | Unexpected surgical findings, Discharge delay |
Behavioral Health / Psychiatry | Admission, Medication administration | Patient de-escalation, Physical restraint event |
Diagnostic / Imaging Center | Patient transport, MRI study | Contrast reaction, Claustrophobic patient |
Emergency Department / A&E | Trauma, Patient admission or discharge, Procedure | Behavioral crisis, Left without being seen |
Emergency Medical Services | Patient transport, Procedure | Patient deterioration, Agitated patient |
Infusion Center | IV access, Medication administration | Allergic reaction, Medication delay |
Intensive Care Unit | Intubation, Admission process, Transport | Family meeting, Cardiac arrest |
Inpatient Unit | Admission process, Medication administration | Patient fall, Discharge process |
Neonatal ICU | Newborn delivery, Central line placement | Parent distress, Infant deterioration |
Obstetrics / Labor & Delivery | Routine delivery, C-section | Postpartum hemorrhage, Shoulder dystocia |
Operating Room | Surgery, OR-to-PACU handoff | Equipment malfunction, Case delay |
Outpatient Clinic | Patient visit, Prescription refill | Difficult news, Patient complaint |
Pediatric Unit | Admission process, Discharge teaching | Behavioral escalation, Parent conflict |
Post-Anesthesia Care Unit | OR handoff, Pain management | Delayed emergence, Uncontrolled pain |
Rehabilitation Unit | Therapy session, Mobility assessment | Patient fall, Delayed discharge |
Teams should debrief often enough that the process becomes a routine communication habit. The goal is not just more conversations. The goal is better conversations that lead to improvements. Mature programs choose debriefing triggers that occur often enough so that debriefing becomes a practiced team skill rather than a rare special event, which can feel unfamiliar to participants. Teams that debrief even when there is a perception that "nothing went wrong" still achieve multiple benefits as detailed in the table below. Table 4. Why Teams Should Debrief Events Where Nothing Went Wrong
Category | Why It Matters | What Teams May Discover |
What Worked
| Capture what went right | Hidden adaptations. Smart workarounds. Team strengths. |
Celebrate recoveries and saves | Near misses caught. Harm prevented. | |
Reinforce behaviors worth repeating | Closed-loop communication. Speaking up. Anticipating needs. | |
Move from good to great | Sharper timing. Better coordination. Clearer roles. | |
Identify system strengths | Gratefulness for resources. Processes that made it easy. | |
Team Learning
| Build the habit before the crisis | Faster gathering to debrief. Familiarity with debrief format. Efficient communication exchange. |
Clarify shared understanding | Same facts. Same plan. Same mental model. | |
Strengthen team familiarity and trust | Teammate styles. Communication preferences. Trust under pressure. | |
Normalize speaking up | Every voice is valued. Learning is routine. Continuous psychological safety building. | |
Small Signals
| Surface small friction points early | Small delays. Unclear roles. Equipment gaps. |
Support morale after hard work | Effort noticed. Stress acknowledged. Team pauses and resets before the next patient. | |
Create a feedback loop for leaders | Lowered threshold to communicate between frontline teams and leadership. Reinforced loops of input and response. |
Debriefing only after negative outcomes teaches teams that debriefing is only for failures. Debriefing events regardless of their outcome reframes debriefing as a normal learning organization behavior.
Where Should Teams Debrief?
Where should a clinical debrief take place? Debriefs should occur as close to the point of care as possible, in a space that allows the team to speak candidly without interruption, within the natural geography of the unit where the event occurred.
Proximity matters: physical proximity helps teams reconstruct what happened with greater accuracy, while moving too far away introduces logistical friction that reduces participation rates. There is rarely an ideal debriefing location, but programs should name a practical location that meets most of the qualities in the table below, with one or two backup locations to debrief as well.
Table 5. Choosing a Practical Location for Clinical Debriefing
Location Feature | Ideal Setting | Practical Compromise | Avoid When Possible |
Quiet enough to hear each other | Calm, quiet space with minimal background noise and no interruptions. | Relatively quiet area where team members can hear each other without raising voices. | Loud area where people struggle to hear, focus, or participate. |
Privacy for the team | Fully private space with only debriefing team members present. | Semi-private area where others may pass by but respect the conversation. | Public area where uninvolved staff gather, watch, listen, or interrupt. |
Patient and family privacy | Removed from patients, families, and visitors to prevent details from being overheard. | Nearby space where the team can avoid identifying details if others are too close. | Location where patients, families, visitors, or uninvolved staff may overhear. |
Close to the clinical area | Immediately adjacent to the care area so the team can debrief while details are fresh. | Close enough that key team members can briefly step away without disrupting care. | Too far away, causing the team to disperse or the debrief to be skipped. |
Enough physical space | Comfortable space where everyone can stand or sit and see each other. | Enough room for the core team to gather without blocking care or traffic. | Cramped, obstructive, or unsafe space where participation is difficult. |
Minimal disruption to ongoing care | Allows the team to pause briefly without interfering with other patients or workflows. | Balances a brief debrief with ongoing clinical responsibilities. | Blocks care, interrupts other teams, or creates new operational problems. |
When Should You Debrief? Hot Debriefs, Cold Debriefs, and Timing
When should a clinical debrief take place? Debriefs should occur as soon as it is safe to do so after the event. The longer the delay, the more detail is lost, the more team members disperse, and the harder it becomes to convert the experience into actionable learning. Two formats define the timing spectrum: the hot debrief and the cold debrief.
The hot debrief occurs immediately or shortly after the event, typically starting within minutes but no later than the end of the shift. This clinical debriefing guide focuses primarily on this type of debriefing. The cold debrief occurs days to weeks after the event on a scheduled basis. The 2025 AHA guidelines recommend both formats as complementary approaches. The hot debrief window closes faster than most teams expect. Designate a facilitator in advance with authority to call the debrief before the team disperses. Although the terms hot and cold debriefing may not translate intuitively across all cultural and linguistic contexts, they remain common in the literature and should be adapted to locally meaningful language.
Table 6. Comparison of Hot and Cold Clinical Debriefing
Comparison Domain | Hot Debrief | Cold Debrief |
Timing | Immediately after the event, within minutes to end of shift | Days to weeks after the event |
Scheduling | Unscheduled, ad hoc | Scheduled days to weeks in advance, often cadenced to an organizational rhythm |
Duration | 2-10 minutes | 20-60 minutes |
Format | Brief, informal, standing or bedside | Structured meeting, scheduled in advance |
Purpose | Capture immediate team observations, acknowledge emotions, identify urgent system issues | Deeper analysis of contributing factors, broader participation, objective data review |
Facilitator | Team leader, charge nurse, or attending physician | Quality officer, unit director, or trained debrief facilitator |
Participants | Available team members at the time of the event | Broader team, may include staff not present at the event |
Documentation | Brief note in debrief log or safety event system | Formal debrief summary, PSO-protected if applicable |
Best for | Resuscitations, rapid deteriorations, procedural events, near misses | Sentinel events, adverse outcomes, complex system failures |
Common alternative names | Immediate debrief, stat debrief, real-time debrief, proximal debrief, post-event debrief, acute debrief, hotwash, after-action review (AAR) | Delayed debrief, retrospective debrief, case review, M&M review, after-action review (AAR) |
How Do You Run a Clinical Debrief?
You run a clinical debrief by moving through three phases: Activation, Conversation, and Translation. This three-phase structure is the foundation of the ACT Debriefing Framework operationalized in a structured, eleven-step DEBRIEF LOOP pathway in Table 7 below. Both the ACT Debriefing Framework and the DEBRIEF LOOP pathway were developed by Dr. Paul Mullan at StatDebrief.
The three phases can be understood as follows:
Activation. The debrief begins the moment a team member recognizes a trigger event or learning opportunity. The goal is not a perfect debrief but a reliable habit of learning from work as it actually happened. Gather available team members, move to a nearby location, and frame the conversation as being about learning, not blame.
Conversation. Begin with a brief reconstruction of the event when needed. Move through the plus-delta questions, then explore contributing factors from a system and team-based perspective. The most effective debriefings limit individual-based feedback. Advocacy-inquiry and other advanced techniques have been studied primarily in simulation settings.
Translation. Convert the conversation into action across three channels: immediate fixes, routed issues requiring escalation to a named owner with a tracked timeline, and team support for any emotional or practical needs. The loop is not closed until frontline staff hear back from leadership on what was done, what could not be done, and why. See the StatDebrief guide on closed-loop communication in healthcare for implementation details. This final Translation step is what distinguishes a program that builds trust from one that simply extracts information and goes silent. Table 7. The DEBRIEF LOOP: Eleven Steps in the ACT (Activation, Conversation, Translation) Clinical Debriefing Framework
DEBRIEF LOOP Step | What Actions Occur in This Step | Related Quality and Safety Concepts |
ACTIVATION | ||
D - Detect the event | Recognize that a clinical event, trigger, concern, near miss, or learning opportunity should prompt a debrief. | Trigger events; near misses; learning opportunities; patient safety events |
E - Engage the team | Gather the available people who were involved or have useful perspectives. | Team-based care; frontline engagement; interprofessional teamwork |
B - Briefing: begin with purpose and ground rules | Briefly state why you are debriefing, how long it will take, and that the goal is learning, not blame. | Psychological safety; learning organization; just culture |
CONVERSATION | ||
R - Reconstruct what happened (*if needed) | Create a shared description of the event: what happened, what was expected, and what actually occurred. | Work-as-imagined vs. work-as-done; shared mental models |
I - Invite open-ended analysis | Use a simple plus-delta framework: ask what went well and what could be improved next time. | Plus-delta debriefing; advocacy-inquiry; reflective practice |
E - Explore contributing factors | Discuss issues that affected the event, including systems, communication, workflow, environment, staffing, equipment, policies, and latent safety risks. | Systems thinking; human factors; latent safety threats; HRO principles; root-cause analysis |
F - Formulate clear takeaways | Summarize the most important themes, lessons, risks, and opportunities for improvement. | Actionable intelligence; knowledge translation |
TRANSLATION | ||
L - Launch immediate fixes | Do what can be safely fixed now: restock, clarify, repair, notify, clean up, update a whiteboard, or prevent recurrence during the same shift. | Real-time improvement; immediate corrective action; agile problem solving |
O - Offer support | Ask whether anyone needs immediate emotional, physical, or practical support, such as a break, handoff, peer support, occupational health, or employee assistance resources. | Second victim phenomenon; employee wellness; healthcare workforce satisfaction |
O - Offload system issues to accountable owners | Route unresolved systems issues to the appropriate leader, manager, committee, safety process, or accountable owner. | Accountability; action tracking; patient safety reporting; risk management |
P - Provide feedback to the team | Close the loop by telling frontline staff what was heard, what was done, what could not be done, and why. | Closed-loop communication; feedback loop; continuous improvement; safety culture |
Structured Models: DISCERN, INFO, STOP5, and When Simulation Frameworks Fall Short
What structured tools are available to guide a clinical debrief? Structured tools available to guide a clinical debrief include DISCERN, INFO, STOP5, TALK, ACED, TAKE STOCK, and several others developed specifically for clinical settings, each differing in trigger profile, setting, length, and training requirements.
Most clinical event debriefing tools share a similar structure: briefly set expectations, review what happened, identify what went well, surface improvement opportunities, and clarify next steps. For program leaders, the most important point is practical: the best debriefing tool is the one your team will actually use consistently. Simulation frameworks can still be useful for trained facilitators but may be too long, education-focused, or instructor-dependent for real-time clinical environments.
Table 8. Selection of Published Structured Tools for Clinical Event Debriefing
Tool | Acronym or Meaning | Setting or Context | Trigger Events |
Debriefing In Situ Conversation after Emergent Resuscitation Now | Pediatric ED / Resuscitation care | Cardiac arrest, defibrillation, intubation, seizures, other critical events | |
Immediate; Not for personal assessment; Fast facilitated feedback; Opportunity to ask questions | Adult emergency departments | Critical ED events; charge nurse-facilitated debriefs | |
Stop for 5 minutes; Summary; Things that went well; Opportunities to improve; Points to action | Emergency department / Resuscitation cases | Resuscitation cases, major trauma, cardiac arrests, deaths, staff-triggered events | |
Target; Analysis; Learning points; Key actions | Operating theatres / Perioperative care | Voluntary clinical self-debriefing after theatre / OR cases | |
Acute Critical Event Debriefing | Pediatric cardiac ICU / CPR events | Cardiac arrests and acute critical events | |
TAKE STOCK hot debrief tool | Pediatric emergency department | Selected significant ED clinical events | |
Debriefing In Situ COVID-19 to Encourage Reflection and Plus-delta in Healthcare After Shift Ends | Emergency departments during COVID-19 | End-of-shift COVID-related clinical learning | |
Debriefing in Suspected COVID-19 to Encourage Reflection and Team Learning | Pediatric hospital / Suspected COVID-19 care | Suspected COVID-19 clinical events | |
Clinical Event Debriefing Instrument | Level-I and Level-II trauma center ED | Clinical events in an emergency department / trauma center setting | |
Multidisciplinary clinical debriefing process after behavioral health emergencies | Pediatric ED and inpatient children's hospital setting | Behavioral health emergencies involving physical restraint | |
Structured, targeted debriefing after intubation | Pediatric emergency department | Pediatric endotracheal intubations |
How to Manage Emotional Debriefings and Traumatic Clinical Situations
How should facilitators manage emotional responses during a clinical debrief? While most clinical debriefings will not involve significant emotional distress, facilitators should monitor for signs of distress before, during, and after every debrief and be prepared to adjust their approach accordingly. Teams that debrief routinely develop greater emotional resilience over time by reducing preventable harm, building trust, and reinforcing supportive team processes.
Kolbe and colleagues offer a practical framework for navigating among three different intentions in a debrief:
1. "Debrief to Learn" (the intention in the vast majority of clinical debriefs): Proceed using your standard structure. Monitor continuously for signs of distress: negative mood, angry outbursts, intrusive or distressing memories, dissociative symptoms, or avoidance symptoms. If these are seen, move to Debrief to Manage.
2. "Debrief to Manage" (when distress signals appear): Transition away from learning-oriented debriefing. Listen, acknowledge, and normalize reactions without pressing for specifics. Do not attempt to treat psychological distress. Offer immediate support with locally appropriate resources. To help debriefing facilitators make this mental shift in real time, the SHIFT protocol, a five-step cognitive aid (developed by Dr. Paul Mullan at StatDebrief) is described in Table 9 below.
3. Avoid "Debrief to Treat": Clinical debriefing is not a psychological intervention and should never be used to treat acute stress disorder or PTSD. Refer to mental health professionals when symptoms warrant.
Table 9. The SHIFT Protocol for Identifying and Managing Emotional Distress During a Clinical Debrief. SHIFT stands for: Spot distress, Halt analysis, Identify intention, Focus on support, and Transfer to support.
SHIFT Step | Purpose of the Step | Suggested Facilitator Action |
S — Spot distress | Notice signs that the conversation may no longer be functioning as a learning or operational debrief. | Look for visible distress, withdrawal, anger, hyper-arousal, dissociation, intrusive memories, or inability to continue. Consider saying: "I'm noticing that this debriefing may be difficult for some people to continue." |
H — Halt analysis | Stop probing for details, analysis, or causal explorations. | Pause the debrief-to-learn conversation without ending the debrief or labeling anyone. Consider saying: "Let's pause the debriefing for a moment." |
I — Identify intention | Decide whether to continue learning or shift toward support. | If people are clearly distressed, move to support. If it's unclear, check in and offer a choice to the group. Consider saying: "How is everyone doing in discussing this event? Should we continue debriefing, or stop and shift toward supporting each other?" |
F — Focus on support | Shift from debrief-to-learn to debrief-to-manage. | Stop debriefing and focus on immediate emotional, physical, and practical needs. Consider saying: "Let's shift the focus to support." |
T — Transfer to support | Connect people with the appropriate supports if needed. | Offer peer support, supervisor support, EAP, occupational health, chaplaincy, mental health professionals, or urgent help if safety is a concern. Consider saying: "We have supports available,... including peer support, EAP, or occupational health..." |
The SHIFT protocol helps facilitators recognize when a debrief is no longer functioning as a learning conversation. The goal is not to treat trauma, but to pause analysis, determine if emotional distress is present or not, support the team, and connect distressed staff with the appropriate resources. The goal of clinical debriefing is learning by the team in the moment, not psychological or emotional treatment of the team in the moment.
How Do You Build and Sustain a Clinical Debriefing Program?
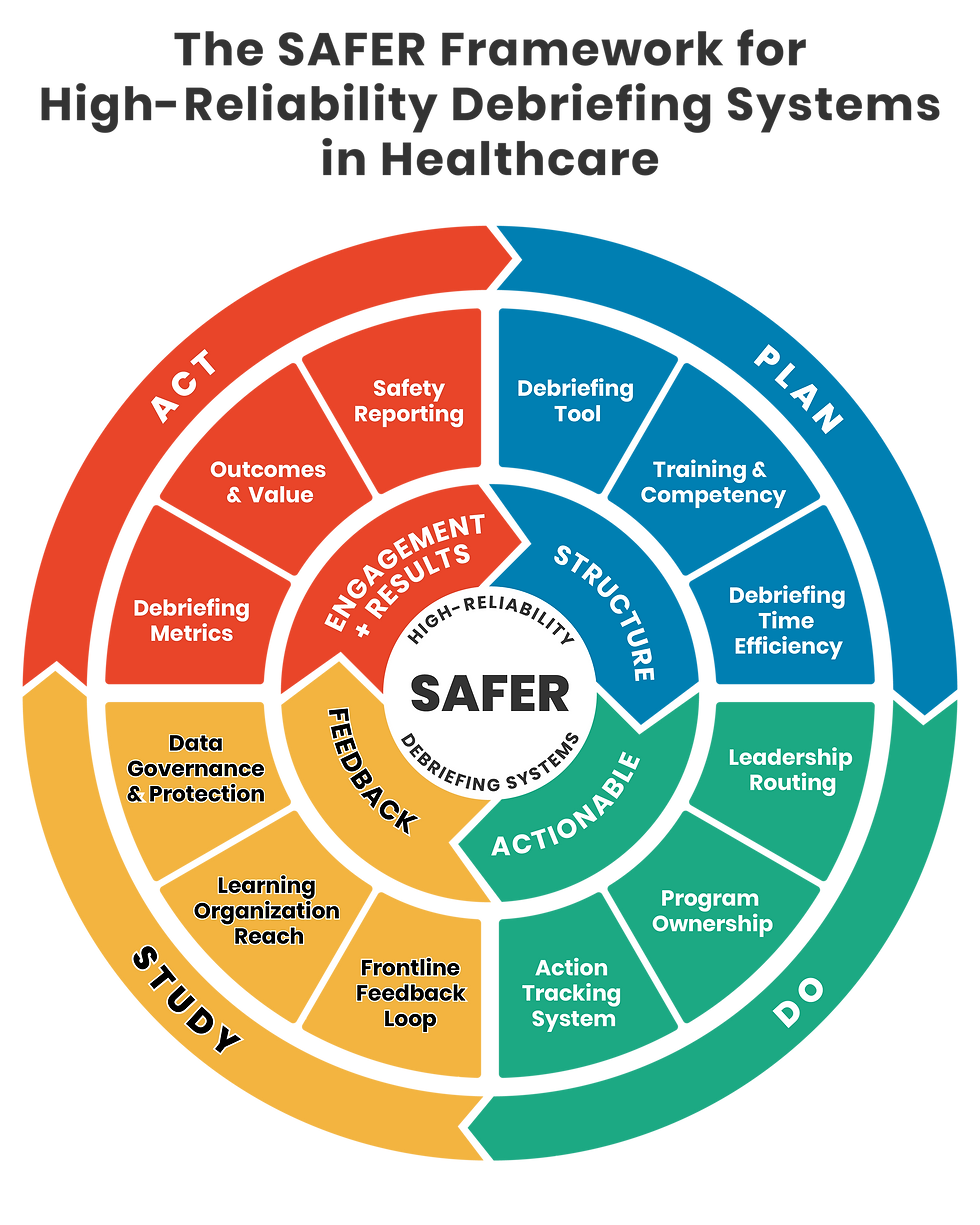
Building and sustaining a clinical debriefing program requires deliberate design across four domains: the structural elements that make debriefing possible, actionable leadership decisions that sustain it, feedback systems that close the loop with frontline teams, and engagement and results metrics that confirm the program is producing value. The SAFER Debriefing System framework (developed by Dr. Paul Mullan at StatDebrief) organizes these domains into a continuous improvement cycle that mirrors the Plan-Do-Study-Act model familiar to every hospital quality leader.
Figure 2. The SAFER Framework for High-Reliability Debriefing Systems in Healthcare.
The SAFER Framework organizes clinical debriefing program maturity across four domains: Structure, Actionable leadership, Feedback, and Engagement/Results, aligned with the Plan-Do-Study-Act improvement cycle.
Structure: How Do You Design a Clinical Debriefing Tool and Train Teams to Use It?
An effective debriefing tool is structured enough to produce consistent learning, simple enough for any team member to facilitate it with a brief training, and brief enough to complete under clinical time pressure.
Before launching your program, the design of your debriefing tool should answer three questions: what scripts or questions the facilitator will cover, in what order, and what will be documented. The plus-delta framework, first used in clinical debriefing with the DISCERN tool created by Dr. Paul Mullan, is the most widely used starting point. Whatever tool is selected, it should be printed, laminated, or digitally accessible at the point of care.
Training teams to navigate the debriefing tool is important. A tool distributed without orientation leads to inconsistent use, inconsistent learning, and program drift. Effective training programs include three components: a brief didactic introduction, at least one observed practice debrief, and ongoing coaching through periodic review of debrief quality by a program champion. Programs with greater training investment produce higher debriefing quality and consistency over time.
Debriefing time efficiency is the third structural variable. The target duration for hot debriefs is 5 to 10 minutes for more complex events, with most clinical events taking only 2 to 4 minutes with the right efficiencies in place. Programs that cannot consistently complete debriefs in under 10 minutes should redesign their tool before addressing any other implementation barrier, as time is the most commonly cited reason teams do not debrief.
Information on how to start incorporating two-minute debriefings into your clinical workflow is available on the World Debriefing Day homepage. World Debriefing Day is an annual event on February 22nd designed to empower healthcare organizations and teams to debrief more frequently and effectively. The World Debriefing Day guide has all the details.
Actionable: How Should Leadership Route, Own, and Track Debriefing Action Items?
How should leadership route, own, and track debriefing action items? Leadership should designate a named program owner, establish an automated routing pathway for debrief findings, and maintain a visible action-tracking system with named owners and deadlines before the first debrief occurs. Without a system to act on findings, debrief insights accumulate without meaningful change. When debriefing findings are lost in a system with no action, participation in debriefings declines, regardless of how well the debrief itself is facilitated.
Leadership Routing: The process for recording key findings and routing them to local leadership should be automated as much as possible. The highest-reliability programs use automated, secure routing with confirmed receipt.
Program Ownership: The clinical debriefing program is typically owned and led by frontline unit leadership in collaboration with organizational quality and safety management. Durable programs require a formal program owner with the role defined in their job description, dedicated time, and accountability measures.
Action Tracking: Clinical debrief action items are tracked by assigning specific tasks to individuals with target deadlines, and progress is made visible through centralized logs, shared spreadsheets, or department communication boards. The highest-reliability programs make action tracking visible to hospital leadership.
Feedback: How Do You Manage and Share Debriefing Data in Healthcare?
How do you manage and share debriefing data in healthcare? Clinical debriefing data should be managed in a secure, confidential, and purpose-built system that protects sensitive information, enables closed-loop communication with frontline teams, and leverages the lessons learned in debriefings to improve healthcare quality and safety across the organization.
Data Governance and Protection: Programs should engage with their legal and risk management teams before launch. In the United States, hospitals should ensure that debriefing is part of their Patient Safety Evaluation System and linked to an AHRQ-listed Patient Safety Organization under the Patient Safety and Quality Improvement Act of 2005, which makes debrief content non-discoverable in legal proceedings. Learn more about the AHDQ Patient Safety Organization. Outside the United States, equivalent protections vary by location.
Frontline Feedback Loop: Teams should receive closed-loop feedback that explains what was heard, what actions were taken, what remains pending, and why certain changes may not be possible. The highest-reliability programs provide feedback consistently and promptly as actions are completed.
Learning Organization Reach: A debriefing program that shares learning only with debrief participants leaves most of its value unrealized. Unit-level sharing benefits staff who were not present. Hospital-wide sharing creates a learning organization. PSO-submitted findings can extend beyond a single hospital into a broader network.
👉🏼 Explore how a PSO can help protect clinical debriefing data and enhance learning. |
Engagement and Results: How Do You Measure Whether Your Clinical Debriefing Program Is Succeeding?
How do you measure whether your clinical debriefing program is succeeding? A high-reliability debriefing program tracks four categories of results: debriefing metrics that capture program activity, patient outcomes that reflect clinical improvement, team member outcomes that reflect workforce impact, and safety reporting rates that signal improvements in psychological safety and safety culture.
Debriefing Metrics — from least to most mature:
Debriefing program exists but no tracking is in place
Quantity only: tracks the absolute number of debriefs completed
Quantity plus percentage: tracks the number of debriefs completed for a given trigger event
Quantity plus descriptors: who debriefs, who leads, when, duration, and debrief themes
Quality of debriefings: discussion depth, efficiency, psychological safety ratings, and facilitator competency scores
Outcomes and Value — from least to most mature:
No outcome evaluation currently in place
Team outcomes only
Clinical outcomes only
Financial or ROI outcomes only
Clinical and team outcomes tracked together
Clinical, team, and financial or ROI outcomes tracked together
Safety Reporting — from least to most mature:
Debriefing occurs only a few times per year, and most staff never report any safety events
Monthly debriefs with one or two safety reports per staff member per year
Weekly debriefs with three to five safety reports per staff member per year
Daily or near-daily hot debriefs with six or more safety reports per staff member per year
Readers can assess where their own program stands across all four SAFER domains using the free SAFER Debriefing System self-assessment.
What Quality Improvement and Learning Organization Frameworks Does Debriefing Support?
Clinical debriefing directly supports and operationalizes many of the major quality improvement and learning organization frameworks, including: High Reliability Organization principles, Kolb's Experiential Learning Cycle, Safety-I and Safety-II, Work as Imagined vs. Work as Done, TeamSTEPPS, the IHI Framework for Safe, Reliable, and Effective Care, and psychological safety theory. Each framework below explains a different dimension of why debriefing works and how to design programs that produce durable learning.
What Are HRO Principles in Healthcare?
HRO principles in healthcare provide a framework to help hospitals and clinical teams anticipate risk, strengthen reliability, learn from frontline conditions, and prevent harm before it reaches patients. A high-reliability organization experiences fewer accidents or harmful events than expected, despite operating in highly complex, high-risk environments. These healthcare organizations focus on creating a culture of safety through 5 principles of high reliability organizations: preoccupation with failure, reluctance to simplify, sensitivity to operations, deference to expertise, and commitment to resilience.
How Does Debriefing Align with High Reliability Organization Principles?
How does clinical debriefing align with high-reliability organization principles? Clinical debriefing operationalizes all five high-reliability principles at the unit level, making it one of the most practical HRO tools for frontline clinical teams. HROs work to create an environment in which potential problems are anticipated, detected early, and addressed promptly to prevent catastrophic consequences. Evidence shows that HRO principles are associated with increased safety and may also positively impact factors affecting the healthcare workforce.
What Is Preoccupation with Failure in Healthcare? Preoccupation with failure in healthcare is the organizational mindset that treats every near-miss, deviation, and unexpected outcome as a signal worth examining, rather than as evidence that the system is working.
Application with Debriefing: Debriefing treats every significant clinical event, including near-misses, as a learning opportunity rather than a minor deviation to move past.
Do: Debrief near-misses using the same structure as adverse events; use trigger lists that include low-harm events; celebrate catches and saves
Don't: Reserve debriefing only for deaths or serious harm; treat near-misses as proof the system worked; skip debriefs when outcomes were good
What Is Reluctance to Simplify in Healthcare? Reluctance to simplify in healthcare is the practice of resisting premature or surface-level explanations for why events occur, and instead probing for the complex system factors, human factors, and latent conditions that actually drove the outcome.
Application with Debriefing: A well-facilitated debrief actively resists simple conclusions, and probes for system-level factors beneath surface-level event descriptions.
Do: Ask follow-up questions when the first answer sounds like individual blame; explore contributing factors across system, team, and process domains
Don't: Accept human error as a root cause without exploring why; allow the most senior person to define what happened unchallenged
What Is Sensitivity to Operations in Healthcare? Sensitivity to operations in healthcare is the ongoing awareness among leaders and staff of the actual state of the systems, processes, and conditions that affect patient care at the frontline, distinct from how those systems are assumed or designed to work.
Application with Debriefing: Debriefing brings leaders into direct contact with frontline accounts of what actually happened, creating real-time operational awareness that dashboards and incident reports cannot fully replicate.
Do: Attend debriefs as a leader and listen without directing; treat debrief findings as primary operational data..
Don't: Rely solely on incident reports for operational awareness; treat debrief findings as anecdotal rather than actionable data
What Is Deference to Expertise in Healthcare? Deference to expertise in healthcare is the organizational practice of valuing and acting on the insights of the staff member with the most direct knowledge of a situation, regardless of their position in the hierarchy.
Application with Debriefing: Debriefs elevate the voice of the frontline clinician who was present and give their account primacy over retrospective administrative reconstruction of the event.
Do: Explicitly invite input from the most junior team members present; protect staff who share critical observations.
Don't: Allow the attending or unit director to summarize what happened before others have spoken; treat seniority as a proxy for accuracy.
What Is Commitment to Resilience in Healthcare? Commitment to resilience in healthcare is the organizational capacity to anticipate potential failures, absorb disruptions when they occur, and adapt and recover quickly enough to prevent catastrophic outcomes.
Application with Debriefing: Regular debriefing builds team capacity to learn from adversity and adapt, forming the behavioral foundation of organizational resilience.
Do: Use debrief findings to update contingency plans and track how often they lead to system changes
Don't: Treat resilience as a personality trait rather than a system property; allow debrief findings to expire without documented follow-through
What Is Kolb's Experiential Learning Cycle in Healthcare?
What is Kolb's Experiential Learning Cycle in healthcare? It is a four-stage framework for adult learning that transforms practical clinical experiences into knowledge, skills, and improved patient care through structured reflection.
Kolb's four stages are concrete experience, reflective observation, abstract conceptualization, and active experimentation. A clinical event is the concrete experience. The debrief is the reflective observation and conceptualization step. The action items that emerge from the debrief represent active experimentation. Without the debrief, teams cycle directly from one experience to the next, missing the reflection that converts raw experiences into learning events.
What Is Safety-I and Safety-II in Healthcare?
What is Safety-I and Safety-II in healthcare? Safety-I in healthcare is the traditional approach to patient safety, focusing on identifying and eliminating things that go wrong. Safety-II in healthcare is an emerging complementary framework that focuses on understanding and reinforcing the things that go right, recognizing that the vast majority of clinical work is performed safely despite significant complexity and constraints.
Clinical debriefing supports both frameworks simultaneously. In a Safety-I context, debriefing surfaces what went wrong and why. In a Safety-II context, debriefing captures the hidden adaptations, workarounds, and team strengths that enabled care to succeed. The plus question in a plus-delta debrief is a direct Safety-II data collection tool. Programs that debrief only after bad outcomes are only practicing a Safety-I mindset. Programs that debrief after routine events, near-misses, and other outcome events are also practicing a Safety-II approach.
What Is Work as Imagined and Work as Done in Healthcare?
What is the gap between Work as Imagined and Work as Done in healthcare? Work as Imagined and Work as Done (WAI and WAD) refers to the gap between how policies and managers expect procedures to be performed and how clinicians actually perform them in practice to manage constraints like time and resources. WAI is the theoretical, ideal procedure, while WAD is the reality, which often involves workarounds that teams develop to get the job done safely. When healthcare is delivered safely, it is not always the result of strictly following all procedures. In many cases, safety is maintained because teams make sensible adjustments in real time to achieve their goals.
Application with Debriefing: Clinical debriefing is the most direct mechanism available for surfacing the WAI versus WAD gap in real time, capturing what frontline teams actually experienced before that knowledge is lost.
Program design implication: Debrief findings that reveal persistent workarounds should be treated as system design feedback. When the same workaround appears across multiple debriefs, it signals that the WAI needs to be updated.
What Is TeamSTEPPS in Healthcare?
What is TeamSTEPPS in healthcare? TeamSTEPPS is an evidence-based teamwork training program developed by the Agency for Healthcare Research and Quality to equip healthcare teams with tools and strategies to improve communication, collaboration, and patient safety.
The TeamSTEPPS 3.0 Pocket Guide identifies three team event tools for learning from clinical work: debriefings, briefings, and huddles. Briefings prepare the team before a case or shift. Huddles address emerging issues in real time. Debriefings capture lessons learned after an event. Together, these tools create a continuous communication cycle that reinforces shared mental models and mutual support.
Application with Debriefing: Clinical debriefing programs that align with TeamSTEPPS terminology reduce the training burden for staff who have already completed TeamSTEPPS training.
Program design implication: Organizations with existing TeamSTEPPS programs should position clinical debriefing as the post-event component of their TeamSTEPPS implementation rather than as a separate initiative.
What Is the IHI Framework for Safe, Reliable, and Effective Care?
What is the IHI Framework for Safe, Reliable, and Effective Care? It is a comprehensive, evidence-based guide from the Institute for Healthcare Improvement that helps health systems achieve operational excellence by organizing the foundational elements of high-quality care into an actionable framework.
The framework highlights the need for healthcare organizations to establish learning systems "characterized by its ability to self-reflect and identify strengths and defects." It specifically calls for organizations to achieve this by "consistently performing agreed-upon team behaviors like briefings and debriefings where the self-reflection occurs." Clinical debriefing is therefore not an optional add-on in the IHI framework. It is named as a required behavioral practice of a learning organization.
What Is Psychological Safety in Healthcare?
What is psychological safety in healthcare teams? Psychological safety is the shared belief among team members that they can speak up about ideas, concerns, or mistakes without fear of punishment, humiliation, or retribution.
Psychological safety is crucial for reducing errors, enabling teamwork, promoting learning, and improving patient safety.Clinical debriefing fosters this safety by providing structured, non-punitive spaces to discuss events. The relationship is bidirectional: psychological safety enhances debriefing's effectiveness, and debriefing builds psychological safety for future honest conversations.
Step-by-Step Preparation Guide for Hospital Leaders
Where should a hospital leader start when building a clinical debriefing program? Start by defining the specific performance gap you want to address through debriefing, then build the program around a measurable aim, and repeated Plan-Do-Study-Act cycles. The tools and frameworks in this article give you everything needed to start moving from assessment to action in a structured sequence.
What Is the Model for Improvement in Healthcare?
What is the Model for Improvement in healthcare? The Model for Improvement, developed by Associates in Process Improvement and adopted by the Institute for Healthcare Improvement, is a framework for accelerating quality improvement in healthcare using three questions combined with rapid Plan-Do-Study-Act (PDSA) cycles to test and implement improvements.
Table 10. Applying the Model for Improvement to a Clinical Debriefing Program
Model for Improvement Question | Application to a Clinical Debriefing Program |
What are we trying to accomplish? | Define the clinical, operational, workforce, or safety outcome you want to improve. |
How will we know a change is an improvement? | Establish baseline rates and track outcome, process, and balancing measures. |
What changes can we make that will result in improvement? | Use debriefings to identify frontline barriers, test solutions, and route system issues to accountable leaders. |
The first question asks to select a clinical, operational, workforce, or system outcome to improve globally, such as reducing inpatient falls, restraint time, surgical complications, nurse turnover, or workplace violence.
What Is a SMART Goal in Healthcare?
What is a SMART goal in healthcare? A SMART goal is a structured objective-setting technique that turns vague intentions into actionable, realistic targets that are Specific, Measurable, Attainable, Relevant, and Time-Bound.
A SMART goal, also known as a SMART aim, is an ambitious goal that teams use to hypothesize how much debriefing will help close a quality gap. Examples include: "Decrease nursing turnover by 10% within 12 months of debriefing program implementation" or "Decrease inpatient falls by 25% within 6 months." The goal is not simply to conduct debriefings. The goal is to use debriefings to discover barriers, identify interventions, and track whether those interventions improve the outcome over time. Table 11. SMART Goal Setting Worksheet for Clinical Debriefing Program Improvement. Use the worksheet below to turn a general debriefing program goal into a specific, measurable aim that can guide implementation and evaluation.
SMART Goal Component | Guiding Question | Your Debriefing Program Aim |
Specific | What clinical, operational, workforce, or safety problem are you trying to improve? | |
Measurable | What baseline and follow-up measure will show whether improvement occurred? | |
Attainable | Is the goal realistic given current staffing, workflow, leadership support, and data access? | |
Relevant | Why does this aim matter to patients, staff, leadership, risk, safety, or quality priorities? | |
Time-Bound | By what date will you evaluate progress? | |
Final SMART Aim Statement | Combine the answers above into one complete aim statement. |
What Is a PDSA Cycle in Healthcare?
What is a PDSA cycle in healthcare? A PDSA cycle in healthcare is a structured, four-stage iterative method used to test small-scale changes for quality improvement. Before your first PDSA cycle, evaluate the current state of your debriefing activities using the SAFER Debriefing Systems self-assessment.
What Is the SAFER Debriefing Systems Assessment?
What is the SAFER Debriefing Systems Assessment? The SAFER Debriefing Systems Assessment from StatDebrief is a high-level, two-minute tool designed for healthcare leaders to evaluate the structure, actionability, feedback, engagement, and results of their clinical debriefing programs.
The assessment is grounded in decades of evidence supporting the effective implementation of debriefing programs by hospital teams. Your baseline score, ranging from 0 to 100, will reveal where your healthcare debriefing program is performing well and where critical gaps exist. Debriefing programs with higher scores have stronger reliability systems in place and are more likely to impact patient, team, and system outcomes.
Once you complete this assessment, you are ready to plan your PDSA cycles. Your debriefing program's first two 30-day PDSA cycles might resemble the examples below. These are basic overviews and will need additional details from the rest of this article to be more comprehensive. For the complete 50-item clinical debriefing implementation checklist, see the StatDebrief resource library. The first PDSA cycle should test whether the debriefing process works in real clinical workflow before expanding it across a larger team.
Table 12. PDSA Cycle 1: Build and Test the Initial Debriefing Process
PDSA Phase | What Hospital Leaders Should Do |
Plan | Assemble a small implementation team. Select the initial target outcome you aim to improve for patients, teams, and/or the system. Design or adapt a rough "version 1.0" of the debriefing tool. Determine trigger events, expected attendees, location, timing, documentation method, and follow-up process. Set a practical aim such as: "Debrief 50% of eligible behavioral events within 6 months." Obtain legal, risk management, privacy, quality, and leadership sign-off before launch |
Do | Pilot the process with a few trained super users. Test the tool in real clinical workflow during the first month. A reasonable early goal might be 10 debriefings to learn how the process works in practice. |
Study | Debrief the debriefings. Review how long they took, whether the right people could gather, where they occurred, what barriers appeared, whether action items were clear, and whether follow-up actually happened. |
Act | Decide whether to adapt, adopt, or abandon parts of the process. Revise the tool, triggers, location, script, data capture, routing process, or leadership response pathway based on what was learned. |
The first PDSA cycle should answer practical questions: Can the team gather? Does the tool fit the workflow? Are action items clear? Does leadership know how findings will be routed and acted upon? The second PDSA cycle should expand participation while strengthening training, tracking, and feedback systems
Table 13: PDSA Cycle 2 — Expand The Debriefing Program Beyond Super Users
PDSA Phase | What Hospital Leaders Should Do |
Plan | Prepare for a broader rollout. Train additional facilitators and clarify expectations. Integrate the debriefing form into existing quality and safety workflows Create a secure database or tracking system for debriefing insights. |
Do | Begin using the process outside the initial super-user group. Encourage debriefing after defined trigger events. Keeping the process brief, practical, non-punitive, and focused on learning how to improve. |
Study | Gather feedback from facilitators, frontline, managers, quality leaders, and risk management. Track debriefing frequency, timing, completion rates, action items, follow-up reliability Monitor any early movement in the target outcome(s). |
Act | Refine the program again. Adjust training, triggers, data fields, routing, feedback loops, and leadership accountability. Continue outcome tracking for debriefing, team, and/or patient outcomes. |
The second cycle shift the program from a champion-driven pilot to a more reliable system. Expansion should prioritize not just volume but also the program's ability to sustain debriefing quality, routing, follow-up, and outcome tracking. The blank PDSA template below can be used to plan the next small test of change, whether the goal is to improve debriefing completion, strengthen follow-up, or expand the program to a new area.
Table 14: PDSA Template for Clinical Debriefing Program Improvement
PDSA Phase | Planning Question | Your Notes |
Plan | What change will you test, where will you test it, and what outcome do you expect? | |
Do | What happened when you tested the change in real clinical workflow? | |
Study | What did the test show, and did the change lead to improvement? | |
Act | What will you adopt, adapt, abandon, or test next? |
Next Steps for Building a Clinical Debriefing Program
A strong clinical debriefing program does not start with a form. It starts with a clear aim, a measurable gap, and a system for turning frontline insights into action. The most sustainable programs treat debriefings not as isolated conversations but as repeatable learning process that helps teams identify problems, test solutions, and improve care over time.
Organizations seeking to strengthen their debriefing infrastructure should study best practices, learn from experienced debriefing leaders, and engage with the broader debriefing community. The field has a long tradition of collaboration, shared tools, and peer mentorship. For U.S. healthcare organizations ready to move from interest to implementation, StatDebrief offers implementation support, PSO-aligned learning systems, and custom technology to help turn frontline insight into measurable improvement.
Ready to build a clinical debriefing program at your organization?
Schedule a 15-minute consultation to discuss your goals, challenges, and how StatDebrief or the Advancing Healthcare Debriefing Quality PSO can support your team:
Frequently Asked Questions About Clinical Debriefing
Q1: What is clinical debriefing?
Clinical debriefing is a structured, reflective conversation held after a real patient care event to help healthcare teams identify what went well, what could be improved, and what should change before the next similar event. It is used in emergency departments, ICUs, operating rooms, inpatient units, outpatient clinics, and other settings where frontline teams need a simple tool for patient safety and team learning. It is not a psychological intervention, a performance review, or a replacement for formal incident reporting.
Q2: What is the difference between a hot debrief and a cold debrief?
A hot debrief occurs immediately after an event, typically within minutes to the end of the shift, while team members are still present and details are fresh. It is brief, usually two to ten minutes, and focuses on immediate learning and team processing. A cold debrief occurs days to weeks later on a scheduled basis, allows for deeper systems analysis, and can include staff who were not present at the event. The 2025 AHA guidelines recommend both formats as complementary approaches rather than alternatives.
Q3: Does clinical debriefing actually improve patient outcomes?
Yes, across multiple clinical settings. A surgical debriefing program at McLeod Health was associated with a 33 percent reduction in 30-day surgical mortality. A pediatric ICU debriefing program at the Children's Hospital of Philadelphia was associated with nearly doubling favorable neurologic survival after cardiac arrest. A pediatric emergency department debriefing program was associated with an 82 percent reduction in restraint time for behavioral emergencies. The evidence is strongest for programs that debrief consistently, document findings, and close the feedback loop with frontline teams.
Q4: How long does a clinical debrief take?
Most hot debriefs take two to ten minutes when a structured tool is used and the team is familiar with the format. Cold debriefs typically 20 to 60 minutes depending on event complexity. Programs that cannot consistently complete hot debriefs in under ten minutes should redesign their tool before addressing other implementation barriers.
Q5: Who should lead a clinical debriefing?
The facilitator should be someone familiar with the debriefing tool and with the interpersonal credibility to foster a psychologically safe conversation for that team. In practice, the facilitator is most often the team leader for that event, the charge nurse, a bedside nurse, a designated debrief champion, or another trained team member. What matters most is not the title but the behavior: opening the conversation with a learning frame, maintaining structure, and ensuring every team member has a chance to contribute.
Q6: How is clinical debriefing different from critical incident stress debriefing?
Clinical debriefing is a team learning conversation focused on quality improvement and systems analysis after a clinical event. Critical incident stress debriefing (CISD) is a structured psychological intervention, facilitated by mental health professionals, designed to reduce the risk of post-traumatic stress disorder after traumatic exposure. A Cochrane review found no evidence that single-session CISD prevents PTSD in healthcare team members and noted possible harm from its compulsory use. Clinical debriefing can identify team members who need referral to psychological support but is not itself a psychological treatment.
Q7: How does clinical debriefing reduce burnout and staff turnover?
Clinical debriefing reduces burnout and staff turnover by providing a structured, safe space to process difficult events, fostering peer support, and improving team communication. Research found that institutional debriefing practices were one of five factors that mitigated the impact of burnout on patient outcomes. A large international survey across 24 countries found that teams that debriefed after resuscitations were less likely to report intention to leave their jobs. Clinical debriefing has not been shown to increase PTSD risk, and most participants report feeling generally better after debriefing. For hospital executives, these findings represent an effective but underused workforce retention strategy. Use the debriefing ROI calculator to model the financial impact at your institution.
HOW THIS ARTICLE WAS WRITTEN
This article draws on peer-reviewed literature identified through PubMed, PMC, and Google Scholar. Sources consulted include AHRQ, CMS, the Joint Commission, the American Heart Association, the Institute for Healthcare Improvement, the American Academy of Pediatrics, ASHRM, and the World Health Organization. All clinical claims were verified against cited sources prior to publication. This article does not constitute legal, regulatory, or compliance advice.
ABOUT THE AUTHOR
Paul C. Mullan, MD, MPH is a pediatric emergency physician with clinical experience across emergency departments, hospitals, and acute care settings in the United States and internationally. He is a quality and patient safety leader and the founder and CEO of StatDebrief and the AHDQ Patient Safety Organization, an AHRQ-listed PSO dedicated to clinical debriefing infrastructure and PSO-protected learning systems. Dr. Mullan helped create the first post-event clinical debriefing program in civilian medicine at Texas Children's Hospital in 2010 and has trained 80+ clinical teams globally in debriefing program design, implementation, and research outputs. He has 50+ peer-reviewed publications on clinical debriefing and related patient safety topics on Pubmed.
HOW TO CITE THIS ARTICLE
Mullan PC. The Clinical Debriefing Guide: What Every Patient Safety Leader Should Know (2026). StatDebrief. Published May 11, 2026. Accessed [insert date]. https://www.statdebrief.com/post/clinical-debriefing-guide
PROPRIETARY FRAMEWORKS
The ACT Debriefing Framework, DEBRIEF LOOP Framework, SAFER Framework, and SHIFT Protocol are proprietary methodologies developed by Dr. Paul Mullan and StatDebrief. Healthcare organizations are welcome to use these frameworks in clinical practice. For training, implementation support, licensing inquiries, or commercial use, contact StatDebrief at info@statdebrief.com.
REFERENCES
Agency for Healthcare Research and Quality. Patient Safety Organization Program.
Agency for Healthcare Research and Quality. Surveys on Patient Safety Culture (SOPS) Hospital Survey.
Agency for Healthcare Research and Quality. TeamSTEPPS 3.0 Program, 2023.
American Academy of Pediatrics. Optimizing Pediatric Patient Safety in the Emergency Department. Pediatrics. 2022;150(5):e2022059673. https://publications.aap.org/pediatrics/article/150/5/e2022059673/189657
American Heart Association. 2025 Guidelines for CPR and Emergency Cardiovascular Care. Circulation 2025 Oct 21;152(16_suppl_2:S284-S312.
American Heart Association. Get With The Guidelines — Debriefing Tools, 2020.
American Society for Healthcare Risk Management. Behavioral Health White Paper Part 3. 2020.
Centers for Medicare and Medicaid Services, 2025. Patient Safety Structural Measure.
CMS Patient Safety Structural Measure: Complete Guide and Hospital Calculator, 2026.
Centers for Medicare and Medicaid Services. State Operations Manual, 2015.
Edmondson A. Psychological safety and learning behavior in work teams. Adm Sci Q. 1999;44(2):350-383.
Institute for Healthcare Improvement. Framework for Safe, Reliable, and Effective Care. 2017. https://www.ihi.org/library/white-papers/framework-safe-reliable-and-effective-care
Institute for Healthcare Improvement, 2020. National Action Plan to Advance Patient Safety.
Institute of Medicine, 1999. To Err Is Human.
Joint Commission. Severe Maternal Hemorrhage. https://digitalassets.jointcommission.org/api/public/content/ed4a0ea369c44adca8bc48ba05b76b61
Joint Commission. https://www.jointcommission.org/en-us/standards/national-performance-goals
Kessler DO, Cheng A, Mullan PC. Debriefing in the emergency department after clinical events: a practical guide. Ann Emerg Med. 2015;65(6):690-8.
Kolbe M, et al. Team debriefings in healthcare: aligning intention and impact. BMJ. 2021;374:n2042.
Lyman KA, et al. The relationship between post-resuscitation debriefings and perceptions of teamwork in emergency department nurses. J Emerg Nurs. 2021 Jul:57:101005.
Mullan PC, Wuestner E, Kerr TD, et al. Implementation of an in situ qualitative debriefing tool for resuscitations. Resuscitation. 2013;84(7):946-51.
Mullan PC, Kessler DO, Cheng A. Educational opportunities with postevent debriefing. JAMA. 2014;312(22):2333-4.
Mullan PC, Zinns LE, Cheng A, et al. Debriefing the Debriefings: Caring for Our Patients and Caring for Ourselves. Hosp Pediatr 2021 Dec 1:hpeds.2021-006339.
Mullan PC, et al. Reducing physical restraints with clinical debriefing.Curr Probl Pediatr Adolesc Health Care. 2023 Sep;53(9):101463.
Mullan PC, et al. Accuracy of Postresuscitation Team Debriefings in a Pediatric Emergency Department. Resuscitation. 2017;70(3):311-9.
PSNet — AHRQ. https://psnet.ahrq.gov/perspective/high-reliability-organization-hro-principles-and-patient-safety
PSNet — AHRQ. https://psnet.ahrq.gov/primer/second-victims-support-clinicians-involved-errors-and-adverse-events
PSNet — AHRQ. https://psnet.ahrq.gov/issue/two-decades-err-human-assessment-progress-and-emerging-priorities-patient-safety
Rose MR, Rose KM. Use of a Surgical Debriefing Checklist to Achieve Higher Value Health Care. J Am Coll Surg. 2018 Sep/Oct;33(5):514-522.
Servotte JC, Welch-Horan TB, Mullan P, et al. COVID-19 Debriefing. Adv Simul (Lond). 2020 Nov 11;5(1):32.
Kolb's Experiential Learning Cycle. https://www.simplypsychology.org/learning-kolb.html
Spencer SA, et al Resuscitation. 2019;142:175-181. https://pubmed.ncbi.nlm.nih.gov/31251894/
Tannenbaum SI, Cerasoli CP. Do team and individual debriefs enhance performance? A meta-analysis. Hum Factors. 2013;55(1):231-245.
World Health Organization, 2012. https://www.who.int/teams/mental-health-and-substance-use/treatment-care/mental-health-gap-action-programme
Zinns LE, O'Connell KJ, Mullan PC, et al. National Debriefing Survey. Pediatr Emerg Care. 2015;31(8):p551-4.


Comments